Part 3: Heart sounds
Sun Jul 12 2026
By B. Hassan

Many cardiac diseases present with pathologic heart sounds and turbulence in blood flow called murmurs. Proper interpretation of these sounds is essential for successful diagnosis. This article first describes heart sounds in the context of normal cardiac physiology and then focuses on the origins of pathologic heart sounds. This article includes embedded videos that include the sounds described, so use a high quality headphones for the best understanding.
Cardiac cycle
The cardiac cycle consists of precisely timed mechanical events that are responsible for rhythmic heart contractions. These events follow the electrical changes in cardiac cells as we talked about in cardiac electrophysiology.
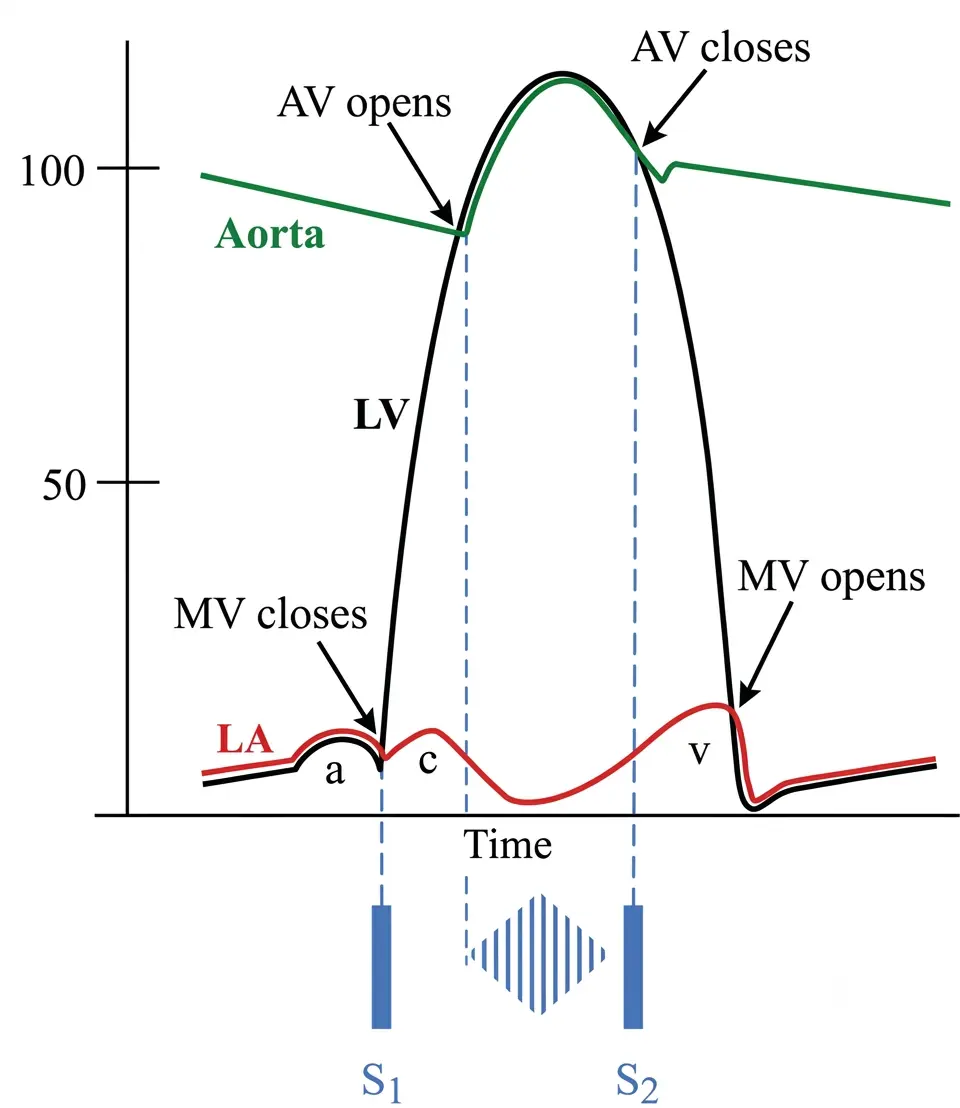
The following diagram describes the pressure changes in the left-sided cardiac chambers during a normal cardiac cycle, and serves as a platform for describing key events.
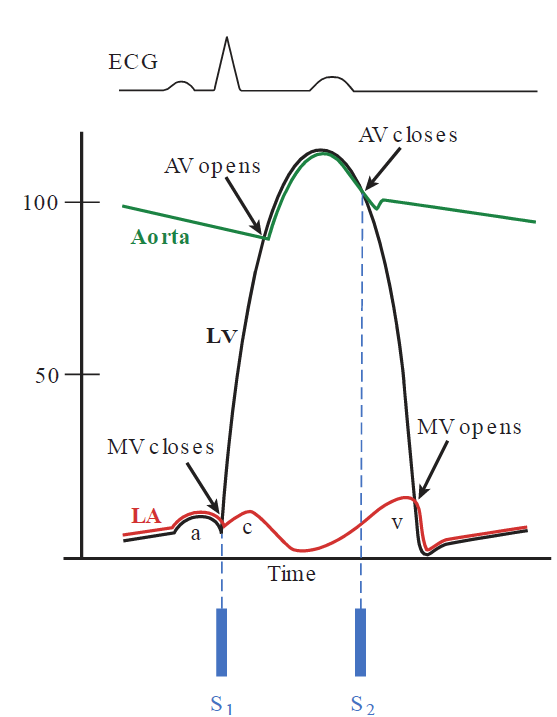
The cardiac cycle can be divided into a systole referring to the phase of ventricular contraction and a diastole referring to the phase of ventricular relaxation and filling.
Throughout the cardiac cycle, blood returns to the right atrium from the systemic circulation. Blood also returns to the left atrium from the pulmonary circulation. During diastole, the mitral valve (MV) is open, making the left atrial (LA) and left ventricular (LV) pressures equal. This causes blood to pass from the atria into the ventricles across the open tricuspid and mitral valves, causing a gradual increase in ventricular pressures.
In late diastole, atrial contraction propels a final volume of blood into the ventricles. This produces a brief additional rise in atrial and ventricle pressures termed the a wave.
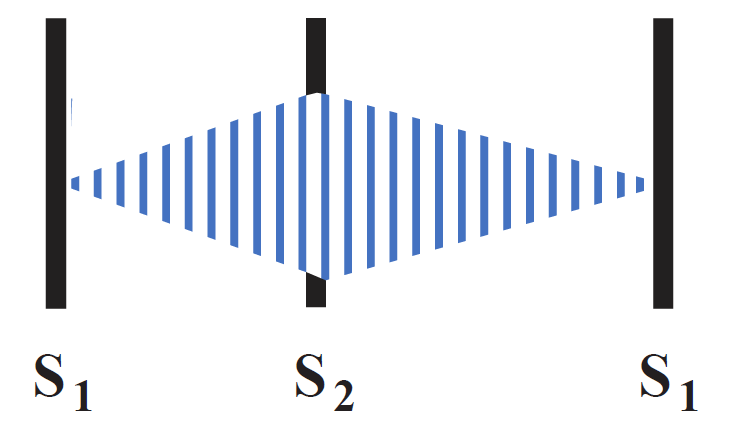
Contraction of the ventricles follows, causing ventricular pressure to rapidly exceed atrial pressures. This results in the forced closure of the tricuspid and mitral valves, which produces the first heart sound known as S1. This sound has 2 nearly superimposed components: the mitral and the tricuspid components. The mitral component may slightly precede the tricuspid component because of the earlier electrical activation of the left ventricle
As the ventricular pressures rapidly rise further, they soon exceed the diastolic pressures within the pulmonary artery and aorta, forcing the pulmonic and aortic valves (AV) to open, and blood is ejected into the pulmonary and systemic circulations.
The ventricular pressures continue to increase during the initial portion of this ejection phase, and then decline as ventricular relaxation starts. Since the pulmonic and aortic valves are open during this phase, the aortic and pulmonary artery pressures rise in parallel to those of the corresponding ventricles.
As the ventricle begins to relax, its pressure falls below the diastolic pressure of the aorta and pulmonary artery. This is because the pulmonary artery and aorta are elastic structures that dissipate pressure more gradually than the ventricles, which is a muscle that relaxes rapidly. This causes the aortic and pulmonary valves to close, producing the second heart sound termed S2. Just like S1, S2 consists of 2 parts: the aortic component referred to as A2 and a pulmonic component referred to as P2. The A2 component normally precedes P2 because the pressure gradient between the aorta and left ventricle is greater than that between the pulmonary artery and the right ventricle, forcing the aortic valve to shut more rapidly.
As ventricular pressure falls further below the pressure of the atria, the tricuspid and mitral valves open, which is a silent event in the normal heart. This is followed by ventricular filling and then the cycle repeats, starting another heart beat.
Systole can be approximated as the period from S1 to S2, and diastole from S2 to the next S1. Although the duration of systole remains constant from beat to beat, the duration of diastole varies with heart rate: the faster the heart rate, the shorter the diastolic phase.
Jugular venous pressure (JVP) curve
This curve is shown in the graph above as a red curve, and represents atrial pressures throughout a cardiac cycle.
The right atrium transmits its pressures to central veins like the jugular vein, and so the right atrial venous pressure curve can be measured using a jugular venous catheter, which serves as an easy measure of the right-side heart functions.
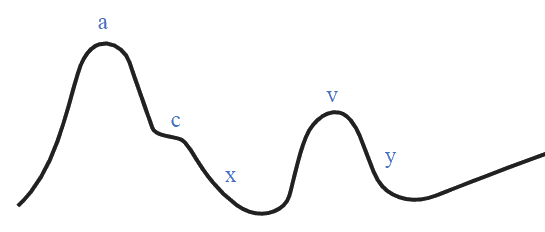
In addition to the a wave we discussed earlier, the LA pressure curve displays 2 other positive waves:
-
The c wave represents a small rise in atrial pressure as the mitral/tricuspid valves close and their cusps bulge into the atrial cavity due to the high pressure in the ventricles.
-
The v wave is the result of blood accumulating in the atria from the pulmonary veins or the vena cava during systole, when the mitral/tricuspid valves are closed.
Note
The c wave may not normally be apparent as its amplitude is generally very small, and so may require sensitive measuring instruments to pick.
Other than the positive waves, 2 negative descents can also be seen:
-
The x wave represents the pressure declining after an a or a c wave.
-
The y wave represents rapid atrial emptying into the ventricles when the mitral/tricuspid valves are open
Diseases that raise the right-sided cardiac pressures (e.g. heart failure, tricuspid valve disease, pulmonic stenosis, pericardial diseases) elevate the JVP, while conditions with reduced blood volume (e.g. dehydration or blood loss) decreases it. In addition, specific diseases can influence the individual components of the JVP, which we will discuss later.
Note
When examining neck veins and JVP, we use the internal jugular vein. Although the external jugular is easier to see, it does not accurately reflect right atrial pressure because it contains valves that interfere with blood flow.
Since the internal Jugular vein is posterior to sternocleidomastoid, we may not see it directly, but we see its effect on the sternocleidomastoid First, observe the pulsations in the skin overlying the internal jugular vein with the patient supine and the head of the bed at 45-degrees. Shining a light obliquely across the neck helps visualize the pulsations.
Pressure volume loop
Another helpful tool to understand the cardiac cycle is the left ventricular pressure-volume loop depicted in the following diagram. It represents the relationship between the volume and pressure in the left ventricle.
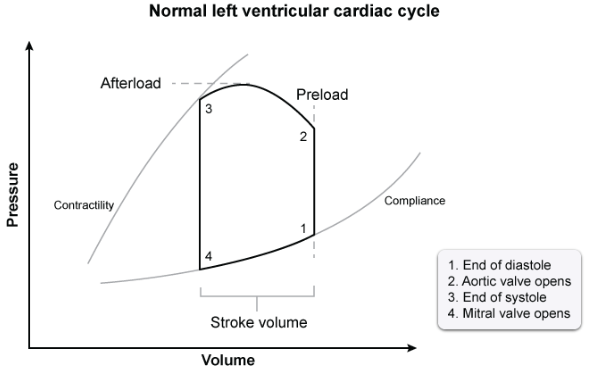
The side from 4 to 1 represents ventricular filling. Here, the volume in the left ventricle increases rapidly, but the pressure only increases little as the ventricular walls stretch to accommodate the blood. At point 1, the mitral valve closes producing S1. This means no further blood can enter the ventricles, and the ventricular volume stays constant.
The side from 1 to 2 represents isovolumetric contraction. Here, the ventricle begins to contract, but its pressure is less than the systemic diastolic pressure, and so the aortic valve stays closed. Since both mitral and aortic valves are closed, blood remains inside the left ventricle, and volume stays constant. At point 2, the ventricular pressure exceeds the opening pressure of aortic valve, and so aortic valve opens.
The volume at point 1 is called the end diastolic volume (EDV), which is the maximum volume of blood in the ventricles just before systole. Higher EDV stretches the heart muscle more, which increases the amount of blood pumped out per beat. This stretching is sometimes referred to as preload.
The part from 2 to 3 represents the ejection of blood by the left ventricle, which causes ventricular volume to decrease rapidly. Pressure rises to a peak, representing the Systolic Blood Pressure and then starts to fall as the squeeze finishes. As the left ventricle squeezes blood, it has to push against the systemic blood pressure, which causes ventricular wall stress, which is sometimes referred to as afterload.
At point 3, the contraction stops, and the aortic valve slams shut, producing S2. The volume at this point is the End Systolic Volume (ESV), which represents the blood left in the heart after full ventricular contraction.
The part from 3 to 4 represents ventricular relaxation. Both valves are closed again, and the heart is relaxing, so pressure plummets, but no blood can enter yet, so volume stays the same. At point 4, the ventricular pressure drops below atrial pressure, and so the mitral valve opens, and the cycle restarts.
The difference between the EDV and the ESV is called the strove volume (SV), which is the amount of blood pumped out by 1 heart beat. The ejection fraction is calculated as the percentage of the EDV the stroke volume is. This represents the fraction of blood pumped out of the left ventricle with each heartbeat.
Ejection fraction =
Heart auscultation
Typical stethoscopes contain two pieces. The concave “bell” piece is meant to be applied lightly to the skin, and accentuates low frequency sounds. Conversely, the flat “diaphragm” piece is designed to be pressed firmly against the skin to eliminate low frequencies and accentuate high- frequency sounds.
Some modern stethoscopes incorporate both the bell and the diaphragm into a single piece. In these models, placing the piece lightly on the skin brings out the low-frequency sounds, while firm pressure accentuates the high-frequency ones.
The following diagram shows the typical cardiac auscultation areas:
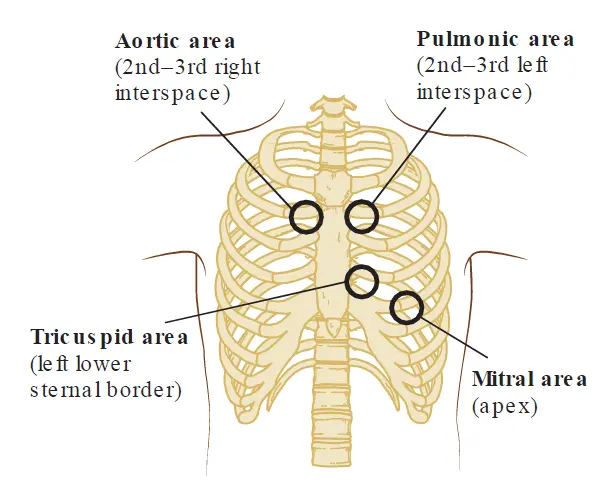
S1
S1 is a high-frequency sound, best heard with the diaphragm of the stethoscope. Although mitral closure usually precedes tricuspid closure, they are separated by only about 0.01 seconds, such that the human ear only distinguishes one sound.
Atrial contraction at the end of diastole forces the tricuspid and mitral valve leaflets apart. They then start to passively drift back together, but once ventricular contraction starts, it causes the ventricular pressure to exceed atrial pressure, forcing the leaflets to shut from whatever positions they occupy at the time.
The main factor that determines the intensity of S1 is the distance between valve leaflets at the start of ventricular contraction. The greater the distance, the more accentuated S1 is, and the shorter the distance, the more diminished the intensity of S1.
Accentuated S1
The distance between the open valve leaflets at the onset of ventricular contraction relates to the PR interval in an ECG, the period between atrial and ventricular contractions. A shorter PR interval causes an accentuated S1 because the valve leaflets have less time to drift back together and are forced shut from a relatively wide distance.
Similarly, in mild mitral stenosis, the valve orifice is narrowed. To squeeze the normal volume of blood through a smaller hole, the pressure inside the left atrium stays elevated throughout diastole. This creates a continuous, high-velocity stream of blood rushing into the ventricle until the very end of diastole, which forces the tips of the mitral valve leaflets wide open and keeps them further apart much longer than normal, resulting an an accentuated S1.
S1 may also be accentuated due to tachycardia because diastole is shortened, and so the leaflets have less time to drift back together before the ventricles contract.
Diminished S1
In first-degree AV block, a diminished S1 results from an abnormally prolonged PR interval. Consequently, following atrial contraction, the mitral and tricuspid valves have additional time to drift back together so that the leaflets are forced shut from only a small distance and the sound is diminished.
In patients with mitral regurgitation, S1 is often diminished because the mitral leaflets may not come into full contact at all.
In severe mitral stenosis, narrow largely-immobile leaflets means the distance between the valve leaflets are decreased while atrial contraction fails to fully open the valve, resulting in diminished S1.
In patients with a “stiffened” left ventricle (e.g. hypertrophic cardiomyopathy), atrial contraction generates a higher-than-normal ventricular pressure at the end of diastole. This greater pressure causes the mitral leaflets to drift together more rapidly, reducing the intensity of S1.
To summarize, a diminished S1 happens in:
- Lengthened PR interval (e.g. first-degree AV block)
- Mitral regurgitation
- Severe mitral stenosis
- Left ventricular hypertrophy (mainly occurs due to prolonged systemic hypertension)
S2
Unlike S1, which is usually heard only as a single sound, the components of S2 vary with the respiratory cycle; they are normally heard as one sound during expiration but become audibly separated during inspiration. This is known as physiologic splitting.
Physiological splitting
Physiological splitting happens because during inspiration, the increased chest volume means the intrathoracic pressure becomes more negative. This negative pressure acts as a suction that pulls blood into the pulmonary circulation, and at the same time decreasing the volume of blood returning to the left side of the heart (since the blood prefers to stay in the lungs at the more negative pressure).
This means that the left ventricle doesn’t have to squeeze as much, and empties its content in a shorter time frame, resulting in an earlier closure of the aortic valve (the A2 component of S2). On the other hand, this pooling of blood in pulmonary vasculature means transiently increased capacitance and decreased impedance of pulmonary vasculature, causing a temporary delay in the diastolic “back pressure” in the pulmonary artery responsible for the closure of the pulmonic valve, and so the P2 component is delayed.
Another factor that contributes to the physiological splitting is that the negative intrathoracic pressure is transmitted to the vena cava, increasing blood return to the right side. Because the right ventricle is now filled with a larger volume of blood, it takes longer for it to empty (prolonged systolic ejection time), further delaying the P2 component of S2.
The combination of an earlier A2 and a delayed P2 during inspiration causes audible separation of the two components. Since these components are high- frequency sounds, they are best heard with the diaphragm of the stethoscope, and splitting of S2 is usually most easily appreciated near the second left intercostal space next to the sternum (i.e. the pulmonic area.)
Abnormalities of S2
Abnormalities of S2 include alterations in its intensity and changes in the normal pattern of splitting. The intensity of S2 depends on the velocity of blood coursing back toward the valves from the aorta and pulmonary arteries after the completion of ventricular contraction, and the suddenness at which that motion is arrested by the closing valves.
In systemic hypertension or pulmonary hypertension, the diastolic pressure in the respective great artery is higher than normal such that the velocity of the blood surging toward the valve increases and S2 is accentuated. Conversely, in severe aortic or pulmonic valve stenosis, the valve leaflets are nearly fixed in position, such that the contribution of the stenotic valve to S2 is diminished.
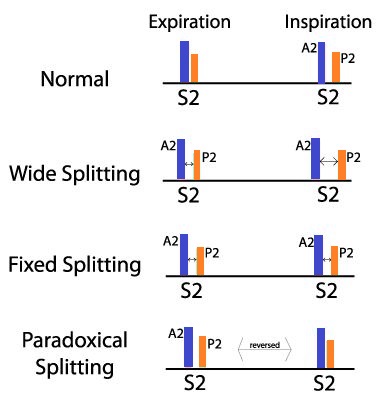
Pathological splitting
There are 3 types of abnormal splitting patterns of S2: widened, fixed, and paradoxical.
Widened splitting of S2 refers to an increase in the time interval between A2 and P2, such that the two components are audibly separated even during expiration and become more widely separated in inspiration. This pattern is usually the result of delayed closure of the pulmonic valve, which occurs in right bundle branch block and sometimes in pulmonic valve stenosis.
Fixed splitting of S2 is an abnormally widened interval between A2 and P2 that remains unchanged throughout the respiratory cycle. This is caused by atrial septal defect, which causes chronic right-sided volume overload (as blood is shunted from the left atrium to the right atrium through the defect). This means that the right side is now constantly filled with a large volume of blood, which means it takes longer to empty its blood (prolonged systolic ejection time), delaying the P2 component of S2, even during expiration. The pattern of splitting does not change during the respiratory cycle because increased filling of the right atrium during inspiration is counteracted by a reciprocal decrease in the shunting through the defect (i.e. the more the blood that returns to the right atrium, the more diminishes the trans-atrial pressure gradient is, and so the less the volume of blood shunted).
Fixed S2 splitting can also be caused by pulmonary hypertension, which increases the resistance (afterload) in the pulmonary arteries. The right ventricle has to work significantly harder and take much longer to squeeze blood against this high pressure, prolonging its emptying time. This causes the pulmonic valve to close much later than the aortic valve, creating a wide split even during expiration.
Paradoxical splitting refers to audible separation of A2 and P2 during expiration that fuses into a single sound on inspiration, which is the opposite of the physiological splitting. It reflects an abnormal delay in the closure of the aortic valve such that P2 precedes A2. In adults, the most common cause is left bundle branch block, which impairs the spread of electrical activity through the left ventricle, resulting in delayed closure of the aortic valve. Then, during inspiration, as in physiological splitting, P2 becomes delayed and A2 moves earlier, resulting in superimposition of the two sounds. In addition to left bundle branch block, paradoxical splitting may be observed under circumstances in which left ventricular ejection is greatly prolonged, such as severe aortic stenosis or hypertrophic cardiomyopathy.
The following video shows split S2 sound, which can be heard as “echoing” of the second heart sound:
Extra heart sounds
Extra heart sounds are heart sounds other than S1 or S2. These sounds are usually abnormal, indicating an underlying pathology.
Extra heart sounds are divided into systolic and diastolic heart sounds. Systolic heart sounds occur during systole, and so are heard between S1 and S2. Diastolic heart sounds, on the other hand occur during diastole, and so are heard between S2 and S1 of the next cardiac cycle.
The following diagram provides a summary of the timings or extra heart sounds
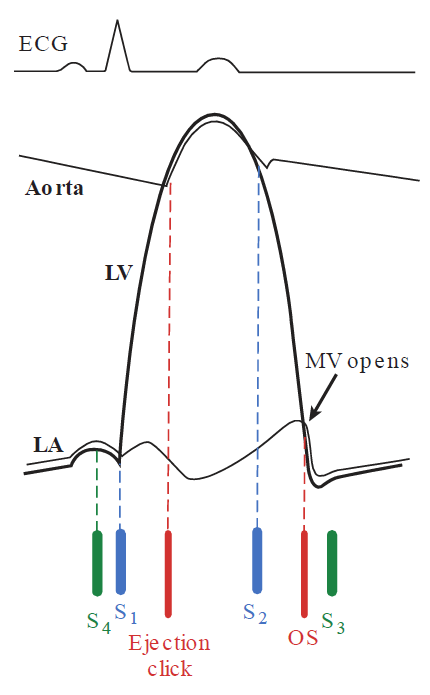
It is not likely that more than one or two of these extra sounds would appear in the same person at the same time, which is helpful clinically because some of these sounds are harder to appreciate if they are superimposed, especially by an inexperienced physician.
Extra systolic heart sounds
Extra systolic heart sounds are clicks that occur during systole (between S1 and S2). They are divided into early, mid, and late systolic clicks.
Clicks occurring in mid or late systole are usually the result of prolapse of the mitral or tricuspid valves, in which the leaflets bulge abnormally into the atrium during ventricular contraction, often accompanied by valvular regurgitation. These are high-frequency sounds, and so they are best heard with the diaphragm of the stethoscope over the mitral or tricuspid auscultatory regions.
Ejection clicks (early systolic clicks)
Ejection clicks are abnormal extra heart sound occurring early during systole shortly after S1 and coincide with the opening of the aortic or pulmonic valves. These sounds are sharp high-pitched snapping sounds, and so they are heard best with the diaphragm of the stethoscope over the aortic and pulmonic areas.
Ejection clicks indicate aortic or pulmonic valve stenosis or dilatation of the roots of pulmonary artery or aorta, which is known as a non-valvular ejection click.
In a stenotic aortic or pulmonary valve, the leaflets are often fused together at their commissures, creating a dome-like shape rather than opening outward flat against the vessel walls. As ventricular pressure shoots up during ejection phase, the stenotic valve is violently forced upward into the aorta or pulmonary artery. But because the leaflets are fused, the valve can only open so far before it reaches its maximum anatomical limit. When the valve leaflets hit this limit, their rapid upward movement is suddenly halted. This abrupt deceleration causes the flexible leaflets to snap, creating a sharp, high-pitched vibration. The moment the valve is forced into its domed position, blood is forcefully ejected through the narrowed stenotic orifice at a very high velocity, which slams against the walls of the root of the aorta or pulmonary trunk. This sudden pressure wave causes a rapid, forceful expansion of the vessel wall, contributing to the resonant snapping sound heard on auscultation.
Note
A helpful analogy for why an ejection click happens in stenotic pulmonary or aortic valve is to think of the valve like a sail on a sailboat. In a normal heart, the sail uncurls smoothly and quietly against the pole. In valve stenosis, the sail is caught by a sudden, violent gush of wind (blood being ejected) and flies upward until it hits the end of its ropes, snapping taut with a loud crack.
In dilatation of the root of the aorta or pulmonary artery, the vessels are abnormally compliant. When the ventricles contract and the normal aortic or pulmonary valve opens, a massive volume of blood is rapidly and suddenly gets ejected into this dilated root (since the normal elasticity that gradually accommodates the blood gets diminished). This sudden, high-velocity surge of blood slams into the vessel wall, and the wall expands instantly until it reaches its structural limit of distensibility and the elastic fibers within the wall are suddenly forced taut.
Aortic ejection clicks are heard at both the base and the apex of the heart and does not vary with respiration. In contrast, the pulmonic ejection click is heard only at the base, and its intensity diminishes during inspiration.
The following video shows an ejection click, followed by an ejection murmur. We will talk about ejection murmurs later, but at this point, just focus of the ejection click
Extra Diastolic Heart Sounds
Opening snap (OS)
Opening of the mitral and tricuspid valves is normally silent, but mitral or tricuspid valvular stenosis produces a sound known as a snap, when the affected valve opens. The sound is produced as a result of the sudden arrest of opening of the stenotic valve.
It is a sharp, high-pitched sound, and so best heard with the diaphragm of the stethoscope. Also, the timing of the sound doesn’t vary throughout the respiratory cycle.
In mitral stenosis, the snap is best heard between the apex and the left sternal border, after A2, when the left ventricular pressure falls below that of the left atrium.
Because of its proximity to A2, an opening snap can be confused with a widely split S2. However, if an opening snap exists, careful auscultation at the pulmonic area during inspiration reveals 3 sounds occurring in rapid succession, which correspond to A2, P2, and then the opening snap. The 3 sounds become 2 on expiration when A2 and P2 normally fuse.
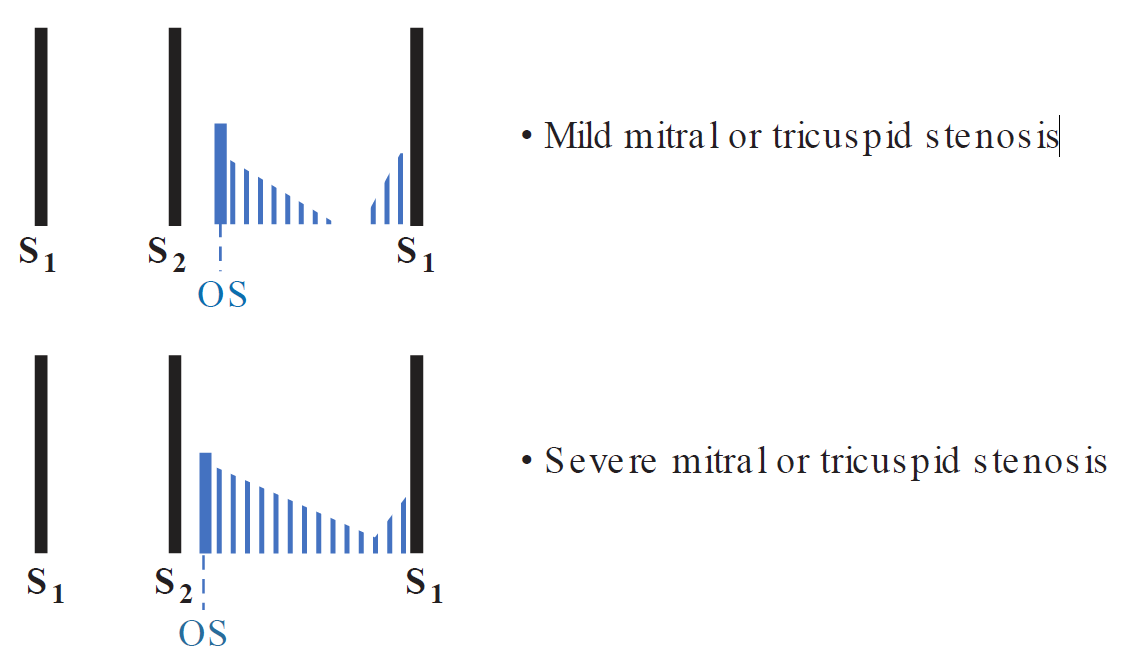
The severity of mitral stenosis can be approximated by the time between A2 and the opening snap. The more advanced the stenosis, the shorter the time interval. This occurs because the degree of left atrial pressure elevation corresponds to the severity of mitral stenosis. The greater the left atrial pressure, the earlier the opening snap occurs.
The following video shows an OS:
Third Heart Sound (S3)
When present, an S3 occurs in early diastole, following the opening of the mitral and tricuspid valves, during ventricular filling.
It is a dull, low-pitched sound, so it is best heard with the bell of the stethoscope. A left-sided S3 is typically loudest over the cardiac apex while the patient lies in the left lateral decubitus position. A right-sided S3 is better appreciated at the lower left sternal border.
Occurrence of the S3 sound appears to result from tensing of the chordae tendineae during rapid filling and expansion of the ventricle. This usually indicates overfilling of the ventricles.
An S3 is physiological in children, young adults, pregnant women, or athletes.
Conversely, when heard in non-athletic non-pregnant middle-aged or older patients, an S3 is a sign of an underlying pathology causing a dilated ventricle. A pathologic S3 is sometimes referred to as a ventricular gallop.
The most important causes of ventricular gallop are:
- Systolic heart failure (HFrEF)
- Dilated cardiomyopathy
- Mitral/tricuspid regurgitation
- Aortic/pulmonic regurgitation
In systolic heart failure, a weakened ventricle only pumps a small portion of blood received (ejection fraction is severely reduced), which causes the ventricles to be distended with blood.
In mitral/tricuspid regurgitation, a sizable portion of blood received by the ventricle gets pumped into the atria, where it is then moves from the atria into the ventricles during the next ventricular filling phase, increasing end diastolic volume and causing the ventricles to be overdistended with blood.
Similarly in aortic/pulmonic regurgitation, blood from the systemic or pulmonary circulations move into the ventricle during diastole, increasing end diastolic volume and causing the ventricles to be overdistended with blood.
Fourth Heart Sound (S4)
When an S4 is present, it occurs in late diastole and coincides with contraction of the atria, occurring when the atria are ejecting blood into a stiffened ventricle. Thus, an S4 usually indicates an underlying pathology, specifically, it indicates a decrease in ventricular compliance.
An S4 is a dull, low-pitched sound and is best heard with the bell of the stethoscope. In the case of left-sided S4, the sound is loudest at the apex, with the patient lying in the left lateral decubitus position.
S4 is sometimes referred to as an atrial gallop.
The most important causes of S4 are:
- Diastolic heart failure (HFpEF)
- Long-standing HTN (left ventricular hypertrophy)
- Aortic stenosis (left ventricular hypertrophy)
- Hypertrophic cardiomyopathy
Diastolic heart failure is usually a symptom of an underlying disease causing ventricular stiffening. It points to the inability of the ventricles to accommodate and carry a normal amount of blood (i.e. diminished end diastolic volume).
Long-standing hypertension causes left ventricular hypertrophy, causing ventricular stiffening. This is also the case on the right side; long-standing pulmonary hypertension causes right ventricular stiffening and an S4 on the right side.
Similarly, aortic or pulmonary stenosis means the ventricles have to push harder to contract harder to push the blood through the narrowed valve orifice. Over time, this causes ventricular hypertrophy and stiffening, producing an S4 on the corresponding side.
The following video compares and contrasts an S3 and an S4:
Quadruple Rhythm or Summation Gallop
In a patient with both an S3 and S4, the 4 heart sounds produce a quadruple beat. If a patient with a quadruple rhythm develops tachycardia, the shortening of diastole duration causes thS3 and S4 to combine, producing a summation gallop that is heard as a long mid-diastolic sound, often louder than S1 and S2.
Pericardial Knock
A pericardial knock is an uncommon, high-pitched sound that occurs in patients with severe constrictive pericarditis. It appears early in diastole soon after S2 and can be confused with an opening snap or an S3. However, the knock appears slightly later in diastole than the timing of an opening snap and is louder and occurs earlier than a ventricular gallop.
It results rom the abrupt cessation of ventricular filling that occurs when the expanding ventricle meets a rigid pericardium in early diastole, which is the hallmark of constrictive pericarditis.
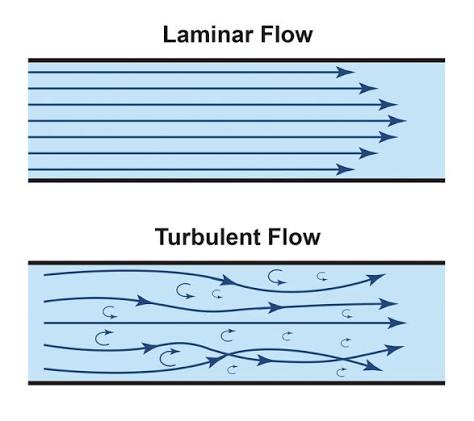
Murmurs
A murmur is the sound generated by turbulent blood flow. Under normal conditions, the movement of blood through the vascular bed is laminar, smooth, and silent.
Murmurs result from any of the following mechanisms:
-
Blood flow across a partial obstruction (e.g. valve stenosis)
-
Increased flow through normal structures (e.g. high-output states, such as anemia)
-
Ejection into a dilated chamber (e.g., aortic aneurysm)
-
Regurgitant flow across an incompetent valve
-
Abnormal shunting of blood from one chamber to a lower-pressure chamber (e.g., ventricular septal defect)
Describing a murmur
Murmurs are described by their timing, intensity, pitch, shape, location, radiation, and response to maneuvers.
Timing refers to whether the murmur occurs during systole, diastole, or is continuous.
The intensity of a murmur is typically quantified by a grading system. In the case of systolic murmurs:
- Grade 1/ 6 (or I/VI): Barely audible (i.e. medical students may not hear it!)
- Grade 2/ 6 (or II/VI): Faint but audible
- Grade 3/ 6 (or III/VI): Easily heard
- Grade 4/ 6 (or IV/VI): Easily heard and associated with a palpable thrill
- Grade 5/ 6 (or V/VI): Very loud; heard with the stethoscope lightly on the chest
- Grade 6/ 6 (or VI/VI): Audible without the stethoscope directly on the chest wall
In case of diastolic murmurs:
- Grade 1/ 4 (or I/ IV): Barely audible
- Grade 2/ 4 (or II/ IV): Faint but immediately audible
- Grade 3/ 4 (or III/ IV): Easily heard
- Grade 4/ 4 (or IV/ IV): Very loud
Pitch refers to the frequency of the murmur. High-frequency murmurs are caused by large pressure gradients between chambers. Low-frequency murmurs imply less of a pressure gradient between chambers.
Shape describes how the murmur changes in intensity from its onset to its completion. For example, a crescendo–decrescendo murmur means the murmur first rises and then falls in intensity. A decrescendo murmur means the murmur begins with its maximum intensity and then the intensity decreases. A uniform murmur doesn’t change intensity over time.
Location refers to the area where the murmur has maximum intensity. This is usually described in terms of the specific auscultatory areas we talked about earlier.
From their primary locations, murmurs are often heard to radiate to other areas of the chest, usually in the direction of the turbulent blood flow.
Finally, similar types of murmurs can be distinguished from one another by simple bedside maneuvers, such as standing upright, squatting, Valsalva maneuver (forceful expiration against a closed airway), or clenching of the fists, each of which alters the heart’s loading conditions, affecting can the intensity of many murmurs.
Systolic murmurs
Systolic murmurs occur during systole (i.e. between S1 and S2). They are subdivided into systolic ejection murmurs, pansystolic murmurs, and late systolic murmurs.
Ejection systolic murmurs
A systolic ejection murmur begins right after S1 and terminates before or during S2, depending on its severity. The shape of the murmur is of the crescendo–decrescendo type. This murmur is typical for aortic or pulmonic valve stenosis.
The ejection murmur of aortic stenosis is separated from S1 by a short audible gap that corresponds to the period of left ventricular isovolumetric contraction, which is the period after the mitral valve has closed but before the aortic valve has opened.
The murmur becomes more intense as flow increases across the aortic valve during the rise in left ventricular pressure (crescendo part). Then, as the ventricle relaxes, blood flow decreases and the murmur lessens in intensity (decrescendo part) and finally ends prior to A2. The murmur may be immediately preceded by an ejection click, especially in mild forms of aortic stenosis.
Although the intensity of the murmur does not correlate well with the severity of aortic stenosis, other features do. For example, the more severe the stenosis is, the longer it takes to force blood across the valve orifice, and the later the murmur peaks. Also, the greater the degree of stenosis, the more diminished S2 is as we discussed earlier.
In aortic stenosis, the murmur is of high-frequency reflecting the sizable pressure gradient across the valve. This means it is best heard using the diaphragm of the stethoscope at the aortic area. The murmur also radiates to the neck but often can be heard in a wide distribution, including the heart apex.
In pulmonic stenosis, the murmur may extend beyond the A2 sound (unlike in aortic stenosis). That is, if the stenosis is severe, it will result in a prolonged right ventricular ejection time, elongating the murmur, which will continue beyond A2 and end just before P2. It also doesn’t radiate as widely as aortic stenosis.
Young adults often have benign systolic ejection murmurs (also termed “innocent murmurs”) resulting from increased systolic flow across normal aortic and pulmonic valves. This murmur often diminishes or disappears completely when the patient sits upright.
The following video shows an aortic stenosis ejection systolic murmur:
Pansystolic (holosystolic) murmurs
These murmurs are caused by regurgitation of blood across an incompetent mitral or tricuspid valve or through a ventricular septal defect. These murmurs are characterized by a uniform intensity throughout systole.
As soon as ventricular systolic pressure exceeds atrial pressure (i.e., when S1 occurs), there is immediate retrograde flow across the regurgitant valve or across the ventricular septal defect. Thus, there is no gap between S1 and the onset of the murmurs.
In mitral regurgitation, the murmur is heard best at the apex and has a “blowing” quality, and often radiates toward the left axilla.
In tricuspid regurgitation, the murmur also has a blowing quality. The intensity of the murmur increases with inspiration because the negative intrathoracic pressure increases venous return to the heart, increasing right ventricular stroke volume and increasing the amount of regurgitated blood.
Note
A blowing quality means the murmur sounds similar to the sound produced by blowing into a microphone
In VSD, the murmur may be associated with a palpable thrill across the sternum. The intensity of the murmur does not increase with inspiration, nor does it radiate, which helps distinguish it from tricuspid and mitral regurgitation. The murmur is inversely proportional to the defect size (i.e. the smaller the defect size, the louder the murmur) as a smaller defect creates more turbulence.
The following video shows an aortic stenosis holosystolic murmur:
Late systolic murmurs
These murmurs begin in mid-to-late systole and continue to the end of systole.
The most common example is mitral valve prolapse, which is caused by abnormally elongated mitral valve leaflets that bow into the atrium during ventricular contraction. This makes it such that the valve closes with high ventricular pressure but opens when the pressure begins to decreases, behaving as a late mitral regurge. This murmur is usually preceded by a mid-systolic click.
The following video shows a late systolic murmur of mitral valve prolapse:
This is also another video showing the late systolic murmur of mitral valve prolapse:
Diastolic murmurs
Diastolic murmurs occur during diastole (i.e. between S2 and the next S1). They are divided into early decrescendo murmurs and mid-to-late rumbling murmurs.
Early diastolic murmurs
Early diastolic murmurs result from regurgitant flow through either the aortic or pulmonic valve.
If produced by aortic valve regurgitation, the murmur begins at A2 and terminates before the next S1 in a decrescendo shape. Because diastolic relaxation of the left ventricle is rapid, a pressure gradient develops immediately between the aorta and left ventricle, and the murmur therefore displays its maximum intensity at the start and decreases over time (i.e. decrescendo) as that gradient decreases (LV pressure starts to increase due to the regurgitant blood). The murmur is best heard with the patient sitting, leaning forward, and exhaling.
Pulmonic regurgitation produces a murmur similar to that of aortic regurgitation, but the murmur is best heard at the pulmonic area and its intensity may increase with inspiration.
The following video shows an early diastolic murmur of aortic regurgitation:
Mid-to-late diastolic murmurs
These murmurs result from turbulent flow across a stenotic mitral or tricuspid valve, or less commonly from abnormally increased flow across a normal mitral or tricuspid valve.
If the murmur is due to stenosis, the murmur is preceded by an opening snap. Following the opening snap, the murmur is at its loudest because the pressure gradient between the atrium and ventricle is at its maximum. The murmur then decrescendos or disappears totally as the pressure gradient between atria and ventricles decreases. The degree to which the murmur fades depends on the severity of the stenosis. If the stenosis is severe, the murmur is prolonged. I the stenosis is mild, the murmur disappears in mid-to-late diastole. The murmur than intensifies at the end of diastole when atrial contraction increases flow across the stenotic valve.
Since the pressure gradient across a stenotic mitral valve tends to be fairly low, the murmur of mitral stenosis is low-frequency and is heard best with the bell of the stethoscope at the mitral area (apex), while the patient lies in the left lateral decubitus position. The much less common murmur of tricuspid stenosis is better auscultated at the tricuspid area.
Hyperdynamic states such as fever, anemia, hyperthyroidism, and exercise cause increased venous return, causing increased blood flow across the tricuspid and mitral valves, which can result in a diastolic murmur. Similarly, in advanced mitral or tricuspid regurgitation, the expected systolic murmur can be accompanied by an additional diastolic murmur owing to the increased volume of blood that must return to the ventricle in diastole.
The following video shows a mid-to-late diastolic murmur of mitral stenosis:
This is also another video showing multiple examples of the mid-to-late diastolic murmurs of mitral stenosis:
Continuous Murmurs
Continuous murmurs are murmurs heard throughout the cardiac cycle (including both systole and diastole). These murmurs result from conditions causing a persistent pressure gradient across 2 structures.
An example of such murmur is that of patent ductus arteriosus, which is an abnormal congenital communication between the aorta and the pulmonary artery, causing blood to continuously pass from the high pressure systemic circulation to the lower pressure pulmonary circulation continuously throughout the cardiac cycle.
This murmur begins in early systole, crescendos to its maximum at S2, then decrescendos until the next S1.